


autism
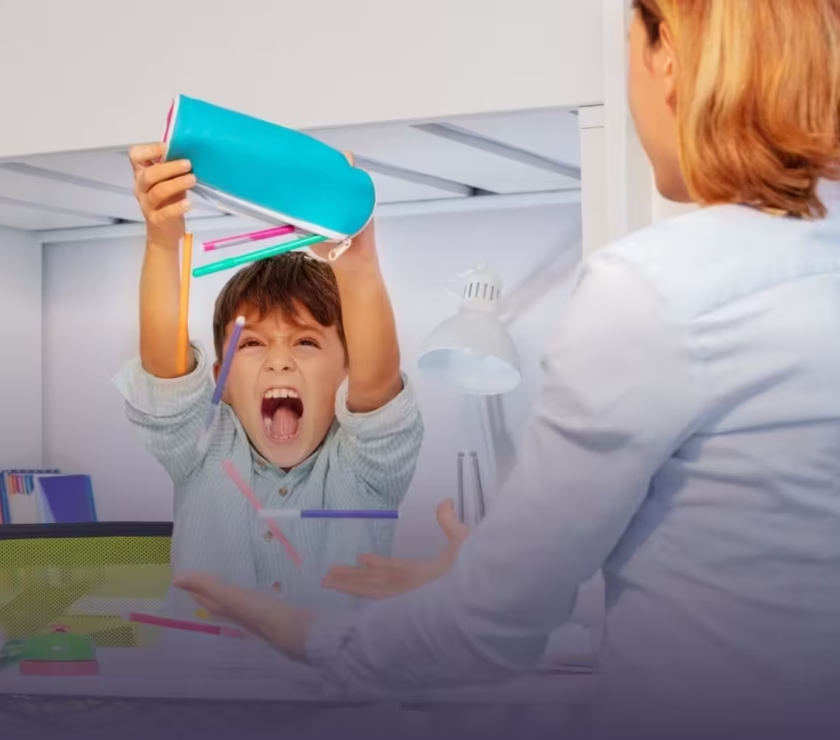
Dinner has become a battlefield. The same five foods. The same plate. The same order. And the moment something changes — a different brand, a new texture, foods touching on the plate — the whole evening derails.
If this sounds familiar, you’re not alone — and you’re not failing as a parent.
Here’s the direct answer: Autism and food aversions are deeply connected. Children with autism are five times more likely to experience significant mealtime challenges than typically developing children, including extremely narrow food selections, ritualistic eating behaviors, and meal-related meltdowns. The root causes are neurological, sensory, and sometimes medical — and this kind of picky eating is fundamentally different from typical childhood pickiness. The good news is that evidence-based interventions, including ABA therapy, occupational therapy, and feeding therapy, have been shown to meaningfully expand the diets of autistic children over time.
This article breaks down why autism and food aversions are so closely linked, what’s actually happening in your child’s body and brain at mealtimes, and which strategies the research supports.
How Common Is Food Selectivity in Autistic Children?
The numbers are striking — and they validate what many families experience as exhausting and isolating.
Studies published in PMC (2006) estimate that 46% to 89% of children with autism have some level of food selectivity (IIDC Indiana University). A separate body of research shows that autistic children are five times more likely to have mealtime challenges — including extremely narrow food selections, ritualistic behaviors (such as foods not touching), and meal-related tantrums — compared to neurotypical peers (Autism Speaks).
A study comparing the eating behaviors of autistic children and typically developing children published in PMC found that autistic children refused 41.7% of foods offered to them, compared to 18.9% in typically developing children. Autistic children also had a significantly more limited food repertoire — an average of 19 foods compared to 22.5 in their peers (PMC, Food Selectivity in Children with ASD and Typically Developing Children).
An important additional finding from research on the SPARK autism study: 16% of more than 113,000 children in the SPARK autism study have a feeding disorder, according to their parents. A separate study of the same SPARK participants found that 1 in 5 autistic children were at high risk for ARFID (Avoidant/Restrictive Food Intake Disorder) — though only 1% had a formal medical diagnosis, suggesting this condition is significantly underdiagnosed (SPARK for Autism).
Why Autism and Food Aversions Are Linked: The Real Causes
Food aversions in autistic children are not behavioral defiance. They stem from multiple interconnected factors — sensory, neurological, gastrointestinal, and behavioral. Understanding each one is key to choosing the right intervention.
1. Sensory Hypersensitivity
The most commonly documented driver of autism-related food aversions is sensory processing differences.
Research published in PMC found that 70% of children with autism chose their food based on texture, compared to only 11% of children without autism (PMC, 2013). For an autistic child, the physical sensation of food in their mouth — its texture, temperature, consistency, and how it changes when chewed — can be genuinely overwhelming or even painful. What feels like a mild mushiness to a neurotypical child may register as something intolerable to an autistic child’s sensory system.
Food aversions driven by sensory sensitivity can involve:
- Texture — mushy, slimy, grainy, or stringy foods
- Temperature — strong preferences for exclusively hot or cold foods
- Smell — heightened olfactory sensitivity that makes certain foods smell intolerable before they’re even tasted
- Color or appearance — aversion to unfamiliar visual presentation, including mixed foods or new brands
- Taste — hypersensitivity to bitter, sour, or spicy flavors
A study published in Frontiers in Pediatrics (2023) using a population-based cohort of 4,930 children tracked ASD symptoms and eating problems from toddlerhood to adolescence, confirming that sensory sensitivities and eating difficulties are bidirectionally linked throughout development (Frontiers in Pediatrics, 2023).
2. Rigidity and Need for Sameness
Autism is characterized by restricted and repetitive behaviors, and this extends to mealtimes. Many autistic children have a deep neurological need for predictability and sameness — and food represents one of the most unpredictable sensory experiences in daily life.
A child may only accept a specific brand of chicken nuggets — not because they’re being difficult, but because a different brand has a slightly different smell, texture, or color that registers as entirely different and unsafe. The same applies to how food is presented on the plate, what utensil is used, or whether family members are seated in the same spots.
This rigidity makes expanding the diet genuinely challenging — because any variation feels like a completely new food to the child’s nervous system.
3. Gastrointestinal Issues
Physical discomfort is a significant but often overlooked contributor to food aversions in autistic children.
Research indicates that nearly 50% of children with ASD report gastrointestinal (GI) symptoms — including constipation, diarrhea, bloating, abdominal pain, and gastroesophageal reflux — compared to 18% of typically developing children (Autism Learning Collaborative).
When a child associates eating — particularly specific foods — with pain or discomfort, they develop conditioned avoidance. Because many autistic children, particularly those who are nonverbal or have limited language, cannot communicate GI pain directly, it often manifests as food refusal, mealtime distress, or escalating selectivity. Parents and clinicians sometimes attribute these behaviors to sensory sensitivity or behavioral inflexibility when there is an underlying medical cause requiring treatment.
4. Anxiety
Anxiety is one of the most common co-occurring conditions in autism, and it directly impacts eating behavior. Fear of trying new foods (neophobia) — or the anticipatory dread of an unpleasant sensory experience — can drive a child to refuse foods they have never actually tried.
Autism Speaks is currently funding a research project specifically examining how anxiety and inflexibility contribute to food selectivity in autistic children, with the goal of developing targeted interventions (Autism Speaks).
5. Oral-Motor Differences
Some autistic children have underdeveloped oral-motor strength — the muscles used for chewing and swallowing. This can make certain textures genuinely difficult to process, leading to gagging, avoidance of foods that require significant chewing, and a preference for softer, less mechanically demanding options. This is a physiological factor, not a behavioral one, and requires targeted oral-motor therapy.
What Autism Food Aversions Actually Look Like at the Table
For families, the daily reality of autism-related food aversions often includes:
- A child who eats fewer than 15–20 foods total
- Strong brand specificity (only one type of chicken nugget, only one brand of crackers)
- Meltdowns when foods touch each other on the plate
- Gagging or vomiting when a non-preferred food is presented
- Refusal to sit at the table if a disliked food is present
- Rituals around food preparation, serving, or utensils
- Anxiety that escalates before meals in unfamiliar environments
- Significant family stress around birthday parties, restaurants, holidays, and school lunches
BCBA Dena Kelly, a feeding therapy specialist, notes that even when a child is not malnourished, food aversions can significantly limit social participation: “For most of us, eating is such a social activity,” she says, noting that parties, summer camps, school lunches, vacations, and restaurants may all become out of the question (SPARK for Autism).
What Helps: Evidence-Based Interventions for Autism and Food Aversions
Managing food aversions in autistic children requires a multi-pronged approach. No single intervention works in isolation, and research consistently points to the value of individualized, interdisciplinary care.
ABA Therapy for Food Aversions
Applied Behavior Analysis (ABA) has a strong evidence base for addressing food aversions in autistic children. A scoping review published in PMC found that studies using ABA consistently reported increased food acceptance and reduced problem behaviors related to feeding (PMC, 2025).
ABA addresses food aversions through:
Functional Behavior Assessment (FBA): Before any intervention begins, a Board Certified Behavior Analyst (BCBA) conducts an assessment to identify the specific causes of food refusal — whether sensory, behavioral, or anxiety-driven — and the environmental factors that maintain it.
Gradual exposure (stimulus fading): Rather than forcing a child to eat unfamiliar foods, therapists introduce new foods systematically and incrementally. This might start with simply having a new food present on the table, then touching the food, then smelling it, then putting it to the lips — all before any eating is expected. This graduated approach respects the child’s sensory threshold and builds tolerance without creating traumatic associations.
Positive reinforcement: When a child tolerates or attempts a new food, they receive meaningful reinforcement — praise, preferred activities, or rewards — that motivates repetition. Over time, this helps the child build positive associations with the food exploration process.
Caregiver training: Consistency between therapy sessions and home environments is essential. ABA programs train parents and caregivers to apply the same strategies at home, ensuring that progress generalizes beyond the clinic setting.
Occupational Therapy (OT)
Occupational therapists address the sensory processing components of food aversion. Research published in PMC on the role of OT in managing food selectivity found that OT combined with sensory integration strategies produced measurable increases in food acceptance and reductions in inappropriate mealtime behavior (PMC, 2021).
OT strategies for food aversions include:
- Sensory desensitization — gradually exposing children to food-related sensory experiences (textures, smells, visual appearances) outside of mealtime to reduce avoidance and distress
- Oral-motor exercises — building the muscular strength and coordination needed for chewing foods of different textures
- Food play — interacting with foods through touching, smashing, or painting without any expectation of eating, which builds tolerance and reduces fear
Feeding Therapy
Specialized feeding therapists — who may be speech-language pathologists, occupational therapists, or BCBAs with feeding training — use structured protocols like the Sequential Oral Sensory (SOS) approach. The SOS approach progresses through a systematic hierarchy of food interactions, from tolerating a food’s presence to eventually eating it, without ever forcing or pressuring.
Addressing the Medical Layer
Before behavioral and sensory interventions begin, families should consult their child’s pediatrician and potentially a pediatric gastroenterologist to rule out or treat underlying medical contributors to food aversion. Treating GI conditions, reflux, constipation, or food allergies may significantly reduce food avoidance behaviors that clinicians and parents had attributed to sensory sensitivity or autism traits alone.
Practical Strategies Parents Can Use at Home
Research from Autism Speaks’ Expert Opinion series, led by Dr. Emily Kuschner (Ph.D., Children’s Hospital of Philadelphia), outlines several home-based approaches:
- Offer control within limits: Present 3–5 options within a category (3 vegetables, 3 proteins) and let the child choose. This reduces anxiety while expanding variety over time.
- Use food exploration, not food pressure: Allow touching, smelling, and looking at a new food before any tasting expectation is introduced. Repeated sensory exposure without pressure helps reduce the novelty response.
- Be patient with repeated exposure: Many children need to be exposed to a food more than a dozen times before they’re willing to eat it. For autistic children, this timeline is often longer. Consistent, low-pressure exposure is more effective than forcing or incentivizing eating with dessert.
- Keep a food diary: Document what your child will and won’t eat, their reactions to specific foods, and any physical symptoms (rashes, GI distress) that appear after eating. This helps clinicians design an accurate intervention plan.
- Don’t use withholding as a strategy: Withholding food until a child is hungry enough to eat has been shown to be dangerous and inappropriate for autistic children and should be avoided (IIDC Indiana University).
When to Seek Professional Help
Not all picky eating in autistic children requires clinical intervention — but some does. Consider seeking an evaluation if your child:
- Eats fewer than 20 foods total
- Has experienced significant narrowing of their diet over time
- Gags, vomits, or becomes distressed when non-preferred foods are present (not just on their plate)
- Is not meeting nutritional needs for growth
- Refuses entire food groups or textures
- Shows mealtime anxiety that is affecting family life, school, or social participation
A multidisciplinary team — including a BCBA, occupational therapist, feeding therapist, and pediatric gastroenterologist — provides the most comprehensive assessment and the best outcomes for autistic children with significant food aversions.
Conclusion: Mealtime Doesn’t Have to Stay This Hard
Autism and food aversions are real, neurologically grounded, and often medically complicated. Your child isn’t being difficult. They’re not “just picky.” And you don’t need to solve this alone.
With the right team, the right assessment, and an approach built around your child’s specific sensory profile and behavioral patterns, meaningful progress is possible. Diets can expand. Mealtimes can become calmer. And families can get their tables back.
At Epic Minds Therapy, every child’s program starts with understanding exactly what’s driving the behavior — not just addressing the surface.
Here’s our invitation: Let’s map out what’s happening at your child’s mealtimes together. Contact Epic Minds Therapy to schedule a consultation with our clinical team. We’ll review your child’s feeding history, sensory profile, and behavioral patterns — and build a plan that actually fits your family.
👉 Schedule a consultation with Epic Minds Therapy. — Serving families across North Carolina.
❓ Frequently Asked Questions
Q: Is picky eating a sign of autism?
A: Picky eating is extremely common in autistic children, but it’s also common in typically developing children. The key differences are severity, duration, and scope. Autism-related food selectivity tends to be significantly more restrictive than typical childhood pickiness, often extending well beyond early childhood, and is driven by sensory sensitivities, rigidity, anxiety, and sometimes GI discomfort. Research shows autistic children are five times more likely to experience significant mealtime challenges than neurotypical peers.
Q: Why does my autistic child only eat certain textures of food?
A: Texture selectivity is the most commonly documented form of autism-related food aversion. Research published in PMC found that 70% of autistic children chose their food based on texture, compared to 11% of neurotypical children. The sensation of food in the mouth — its consistency, how it changes when chewed, how it feels on the tongue — can be genuinely overwhelming for children with sensory hypersensitivity. This is a neurological difference, not a behavioral choice.
Q: How many foods do autistic children typically eat?
A: Research comparing autistic and typically developing children found that autistic children ate an average of 19 foods over a three-day period, compared to 22.5 foods in typically developing children. However, many children with significant food selectivity eat far fewer — some as few as 5–15 foods total. Children who eat fewer than 20 foods are generally considered candidates for clinical feeding intervention.
Q: Can ABA therapy help with food aversions in autism?
A: Yes. A scoping review published in PMC found that studies using ABA consistently reported increased food acceptance and reduced problem behaviors related to feeding in autistic children. ABA addresses food aversions through functional behavior assessment, graduated exposure, positive reinforcement, and caregiver training. It is most effective as part of a multidisciplinary approach that also includes occupational therapy and, when relevant, medical evaluation.
Q: What foods are commonly accepted by autistic picky eaters? A: Autistic children with food selectivity tend to prefer foods with predictable, consistent textures — such as chicken nuggets, French fries, macaroni and cheese, crackers, and plain pasta. Crunchy, dry, or smooth foods are often more tolerated than mushy, mixed, or variable-texture foods. Brand specificity is also common — a child may accept one brand of a food but refuse another with a slightly different appearance or texture.
Q: What should I NOT do when my autistic child refuses food?
A: Avoid forcing a child to eat a food they refuse, as this can create traumatic food associations that worsen aversion long-term. Research from the Indiana Resource Center for Autism specifically identifies withholding food until a child is hungry enough to eat as dangerous and inappropriate for autistic children. Avoid using dessert as a bribe — research indicates this does not help children develop a positive relationship with food and may reinforce mealtime conflict. Gradual, low-pressure exposure is consistently more effective.
📚 Sources
- PMC / NIH — Food Selectivity and Sensory Sensitivity in Children with Autism Spectrum Disorders (2013) https://pmc.ncbi.nlm.nih.gov/articles/PMC3601920/
- PMC / NIH — Food Selectivity in Children with ASD and Typically Developing Children https://pmc.ncbi.nlm.nih.gov/articles/PMC2936505/
- PMC / NIH — Feeding and Eating Problems in Children and Adolescents with Autism: A Scoping Review (2021) https://pmc.ncbi.nlm.nih.gov/articles/PMC8323334/
- PMC / NIH — The Role of Occupational Therapy in Managing Food Selectivity of Children with ASD (2021) https://pmc.ncbi.nlm.nih.gov/articles/PMC8620957/
- PMC / NIH — Treatments for Eating Disorders in People with Autism Spectrum Disorder: A Scoping Review (2025) https://pmc.ncbi.nlm.nih.gov/articles/PMC11932270/
- Frontiers in Pediatrics — Interrelated Development of ASD Symptoms and Eating Problems in Childhood (2023) https://www.frontiersin.org/journals/pediatrics/articles/10.3389/fped.2023.1062012/full
- Autism Speaks — Autism and Food Aversions: 7 Ways to Help a Picky Eater https://www.autismspeaks.org/expert-opinion/autism-and-food-aversions
- SPARK for Autism — Very Picky Eating in Children with Autism https://sparkforautism.org/discover_article/picky-eating-autism/
- Indiana Resource Center for Autism (IIDC / Indiana University) — Mealtime and Children on the Autism Spectrum: Beyond Picky, Fussy, and Fads https://iidc.indiana.edu/irca/articles/mealtime-and-children-on-the-autism-spectrum-beyond-picky-fussy-and-fads.html
- Autism Learning Collaborative — Information on Picky Eating in Children with Autism https://www.autismlearningcollaborative.com/autism-and-picky-eating-what-you-need-to-know/
- Step Ahead ABA — Understanding the Impact of ABA Therapy on Mealtime Challenges in Children with Autism https://www.stepaheadaba.com/blog/the-role-of-aba-therapy-in-addressing-food-aversion-and-mealtime-behaviors
- Discovery ABA — How to Address Food Selectivity and Picky Eating with ABA Techniques https://www.discoveryaba.com/aba-therapy/how-to-address-food-selectivity-and-picky-eating-with-aba-techniques
- Apollo Behavior — Autism and Food Aversion: How ABA Therapy Can Help https://apollobehavior.com/autism-and-food-aversion-how-aba-therapy-can-help/
- Building Blocks Therapy — Autism and Picky Eating https://www.buildingblockstherapy.org/blog/autism-and-picky-eating